Ankle injuries are the most common injury in sports by far, so ankle bracing and taping is a hot topic among the sports community!
Throughout my athletic life, I had the chance to see both: the coach who ensured that every single player would wear ankle braces, and the coach who would do the exact opposite. I would be in one team one year being frowned upon by my coach for not wearing ankle braces, and then be in another the next year where I’d be praised for not wearing them.
At the time I wasn’t sure who to believe, so I decided to do some reading on this topic. If you are in a similar situation as I was back then maybe you can benefit from my insights. I will tell you what I found in the scientific literature, and also give you my educated opinion (read more about What Biomechanists do). Not to say that I have the absolute truth… but at least you will have some information to go with for now to help you decide if external supports are a yea or a nay for you.
External supports are just like most things in life, they have advantages and disadvantages. In this article, I will discuss the pros and cons of external supports for ankle stability as they relate to ankle sprain mechanisms.
We’ll start by discussing how you actually get injured. It’s important to first understand what motions cause these injuries so that we can easily jump right into talking about how these supports work to prevent your ankle from going to injurious postures. Then we will end by talking about how these supports influence your biomechanics… Shall we?
How do you get injured?
An ankle sprain occurs when a person contacts the ground with the foot in the wrong posture (to read more about walking mechanics), and the impact ends up pronouncing those postures to the point where ligaments within the foot get stretched and possibly torn. There are inversion and eversion sprains.
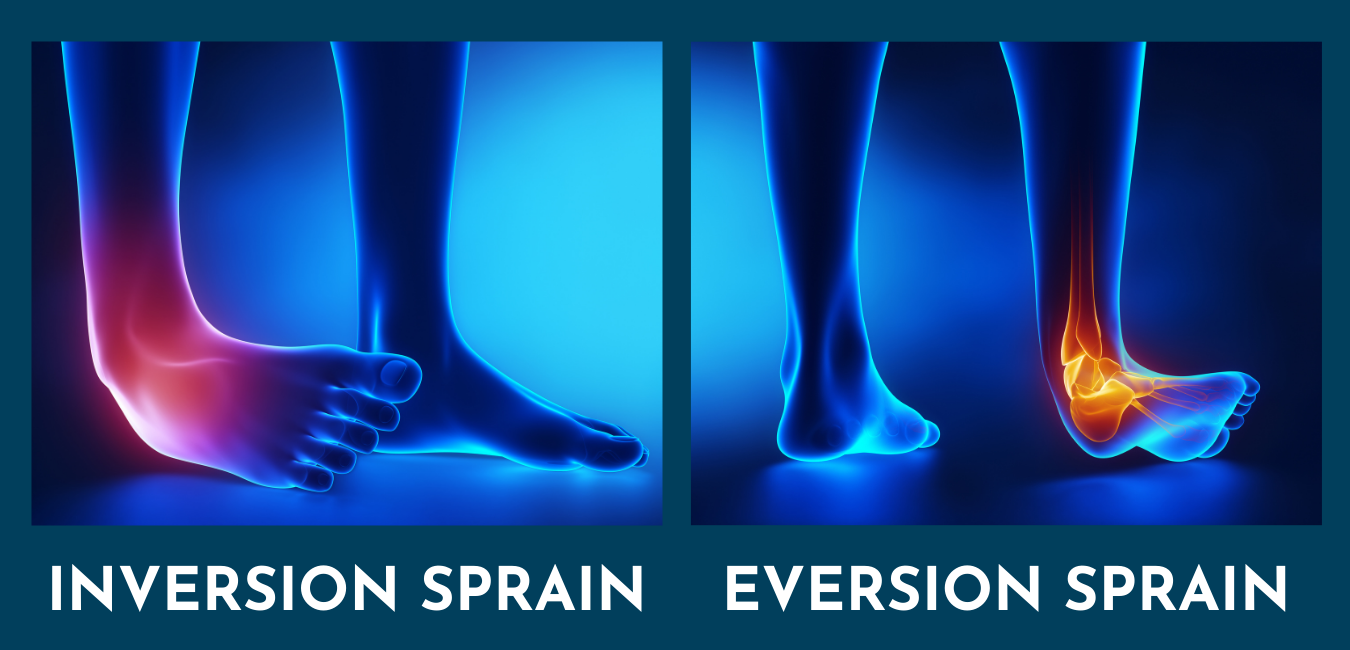
The main 3 postures that are associated with inversion ankle sprains are:
- Plantar flexion,
- Foot inversion (supination of the rearfoot)
- Internal rotation of the foot with respect to the lower leg
The greater the plantar flexion or internal rotation of the foot while your foot is in the air (before contacting the ground) the higher the chances of rolling your ankle. As you can see, your foot posture in the air is key for not getting injured, and your whole neuromuscular system should be continuously adjusting the postures of your feet while in the air to prepare them for contact.

On the other hand, there are also eversion sprains, which are less common but sometimes more serious. These type of sprains are associated with 2 main postures:
- Dorsiflexion
- Rapid eversion
Causes
For any kind of sprain, there are 2 different kinds of “causes”, one of which is mechanical and the other which is related to neuromuscular control.
The mechanical causes refer to things such as ankle laxity, which tends to affect people who may have pathologies which may compromise elasticity of tendons or ligaments, or people who have had previous ankle injuries.
Reduced ligament stiffness reduces ankle stability. However, a large majority of people can benefit from working extra hard to improve muscular strength around the ankle and their proprioceptive function to pick up the slack of lax ligaments. Depending on the severity of their problem and their ability to improve with training, they may benefit from external ankle supports at some point or another, possibly for an indefinite period of time.
Neuromuscular causes on the other hand relate more to the inability to use sensory information to move their ankle to the appropriate postures to prepare it for impact. In this case, proprioceptive training is a must to reduce the risk. Again, depending on their trainability, some people may have to rely on braces or taping longer than others.
Literature Highlights: Bracing & Taping
At some point, it was believed that taping and braces were most effective at decreasing the incidence of ankle sprains among pre-injured athletes. In 2011-2012, Dr. McGuine from the University of Wisconsin tested the effectiveness of ankle braces among high school football and basketball athletes – whether they were previously injured or not. They found a significant correlation between ankle brace use and a reduction in ankle sprain incidence in athletes regardless of whether they were previously injured or not, meaning that anyone could benefit from using braces.
Some data has previously shown that brace use could modify leg mechanics (Gregory et al. 2019 supports this). So Dr. McGuine decided to also test if brace use and knee injuries were correlated. They found no correlation between the two. In other words, if the mechanics of brace wearers changed, the change did not increase their risk of knee injury – at least not at the time of the study. I may point out that long term effects were not tested in this study, and evidence to say either or is limited.
As you can see above, I decided to report mainly on findings related to braces rather than taping because I consider that it is harder to find taping studies with good quality data. I say this because it is much harder to control how each person gets taped. In research, if your goal is to test an intervention, you need to make sure that the intervention is consistent across every athlete. That way, you can be more confident that your results are more likely attributed to the intervention. However, with taping, this is not the case due to different practitioners having different skills or preferred techniques, which may sacrifice taping consistency.
Goals of External Supports
The main mechanical goal of these supports is to restrict ankle motion. The rationale is that if the brace or tape can help you keep a more neutral ankle posture in the air, and give a bit more rigidity at the joint during landing, you may have a lower chance to land in the injurious postures mentioned above. This means that the supports must prevent your foot from going into excessive plantar flexion, foot eversion, or internal foot rotation to avoid inversion sprains, or prevent dorsiflexion in combination with eversion to prevent eversion sprains.
It is also believed that having compression around the joint may improve neuromuscular function, and since tape has direct contact with the skin, it may have a better chance at increasing the effect on neuromuscular function than braces. However, there is some evidence that show that taping does not improve proprioception.

Mechanics:
Structure of External Supports
There are 2 kinds of braces: rigid braces and laced braces. Both types of braces have been reported to be effective at restricting inversion/eversion and plantarflexion/dorsiflexion of the ankle, with the rigid ones providing stiffer support than the laced ones. Then there is taping, which allows customization. Movement restrictions with taping vary depending on the goal of the taping job. For example, if an athlete is at risk of inversion sprains, then the taping job’s focus would be placed on avoiding plantar flexion, inversion, and internal rotation of the foot (talus) with respect to the tibia. Note that internal rotation tends to be more effectively restricted with taping than braces because taping allows a more snug fit than braces.
The other two factors that are important to consider when using tape include the variability in practitioners’ skill and technique repertoire, which may influence the effectiveness of the taping job at a given time. And second, the fact that tape, unlike braces, tends to loosen up after 20-30 min of exercise! If this is the case, it means that tape is only capable of providing mechanical support during the beginning of a game.
There’s no question that these movement restrictions are effective at preventing immediate injury, and that they can be particularly beneficial to anyone who has compromised ankle stability. However, there are some downsides must be considered.
Mechanical Changes
The increased ankle rigidity does modify the mechanics of the entire leg and the consequences may not be too exciting. On the one hand, ankle mobility is crucial for power generation, and if restricted, the ability to generate ankle power can be compromised.
On the other, ankle plantarflexion/dorsiflexion are super important movements to help absorb the impact of the ground at contact. If restricted, ground reaction forces can not dissipate appropriately, resulting in higher force transfer to the body through the adjacent joints (e.g. knee). Although Dr. McGuine did not show a direct correlation between ankle brace use and knee injuries, I think that the other pressing question remains of whether the increased ankle rigidity could increase repetitive compromising loads to the knee in a way that may contribute to more chronic degenerative conditions over time.
To finalize…
I would like to end by recommending a few tips:
- Assess your ankle stability. For this, you may need the help of a professional who can help, such as a sports biomechanist.
- If your stability is compromised, use tape if you have access to someone who can help effectively, or throw a pair of braces that would fit you best.
- Get your biomechanist to prescribe you corrective exercises in a progressive manner to help you withstand the needs of your sport.
- Slowly reduce the external rigidity, either by reducing modifying the tape or by loosening the brace until it starts coming off at times.
- Gradually reduce the amount of time that you spend with the brace or tape on.
- Lastly, but more importantly, ensure that you have the proper advice to guide you! Do what feels right and secure for you.

References
- Am J Sports Med. 2011 Sep; 39(9): 1840–1848.
- Am J Sports Med. 2012 Jan; 40(1): 49–57.
- Asia-Pacific Knee, Arthroscopy and Sports Medicine Society (APKASS). 2018 Apr; 12: 12-16.
- J Athl. Training. 2002; 37(4): 436–445.
- Physiol. Meas. 2019 Apr; 40(4).